
On the one hand, the development of the Omicron narrative indicates concealment that points to important considerations for fighting the virus. On the other hand, its speed of change points to the need for a new (or old) praxis for action.xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
As soon as Omicron was detected in South Africa, the speculation about its origins emerged seemingly almost in full-cloth and was repeated around the world: the new highly mutated form of the COVID-19 disease 'most probably' originated in the body of an unvaccinated immuno-compromised HIV patient somewhere in South Africa, and that because the body was not able to fight off the virus quickly, it remained circulating in their body becoming a 'factory of variants for the whole world'. This, we were told by the LA Times, was 'logical','because of the prevalence of HIV in the region' that coincided with low vaccination rates.

Before Omicron was detected, the global vaccination push had begun to wane as a result of emerging evidence that the vaccines did not prevent transmission1 of the virus, and that they waned in effectiveness2, forcing people into a seemingly open-ended need to boost every 3-6 months in order to maintain a level of antibodies still capable of preventing symptomatic disease, at the least, and severe illness, hospitalization, and death, at the worst. So, it was no surprise that, based on little more than the 'logic' of the origin story, that people still searching for ways to convince others to be vaccinated, rightly or wrongly, seized on it as a means of reinforcing their message. More than this, the argument itself became through this highly mutated and more transmissible: based on long-held fears of a disease that the world has still not found a vaccine for (HIV, for which only cocktails of effective long-term treatments are yet available), the argument aggressively targeted specific holdouts. Now, a single unvaccinated individual could provide the breeding ground for variants that could take down the entire world's population. Furthermore, because of the coincidence of the HIV patient and their location in a mostly unvaccinated Global South country, the argument naturally began to (and still does) focus on 'vaccine inequality' resulting from the hoarding of vaccine in rich countries endlessly boosting3.

Together, two dimensions of the rationale for vaccinating that had been secondary and drowned-out in the deluge of information directed at convincing rich countries' populations to inject the vaccine, took center stage. Omicron has and still is shifting the debate about vaccination from one oriented towards rich countries and broad uptake, to one directed at developing countries of the Global South and those minorities down to individuals in the developed West who still refuse.
But, as we know now, it was only a matter of about a week before it turned out that, in fact, Omicron was already present in test-samples taken about a week before South Africa sounded the alarm. This from CBS News:
Detected in the Netherlands, it didn't take long to confirm that the new variant was present already in other EU-countries and that Botswana had detected the variant in foreign diplomats who entered the country on November 7th, almost a full 3-weeks before South Africa informed the world about it. As, NPR pointed out:
So, just as quickly as the origin story about Omicron arose, it began to unravel. In fact, there is now little talk about the origins any longer, although, interestingly, certain aspects of its logic still linger in the COVID narrative. Take, for instance, this article published in the New York Times on December 19, 2021:
This sentence does two interesting things: first, it hides the fact that vaccines already failed to stop transmission of the virus by re-presenting that fact as now tied exclusively to the widely reported understanding that Omicron itself evades the vaccine; second, no longer tied to a specific origin story, the logic of the story persists: 'unvaccinated could fall more seriously ill, and become a source of new variants'. This 'could' is only partially the 'could' of science: for while it is true that the unvaccinated are vulnerable to more severe illness and death, this is primarily not that 'could' but the pop-cultural 'could' that references recent memory back to the speculation on the HIV patient. That story 'could' be true—it isn't proven, there are counter-vailing facts and reasons to believe it is not true—but it 'could' be true. Together these conflations represent the sort of slight-of-hand innuendo that has defined the COVID narrative throughout the past 2-years. Sure, one can re-write into it the best of intentions, everything that's missing, give it all the benefit of the doubt—but in so doing, you'll have lost your 20-bucks. It really is time to reckon with the reality of the COVID hustle, what it means, and how one should respond to it so that they don't end up duped, broke, or worse, injured.
The Shell Game
Throughout this pandemic 'the science' that has been used to justify lockdowns, social-distancing, vaccination, and masking has followed the same principles. Look at Neil Furguson's COVID death predictions discussed in Nature:
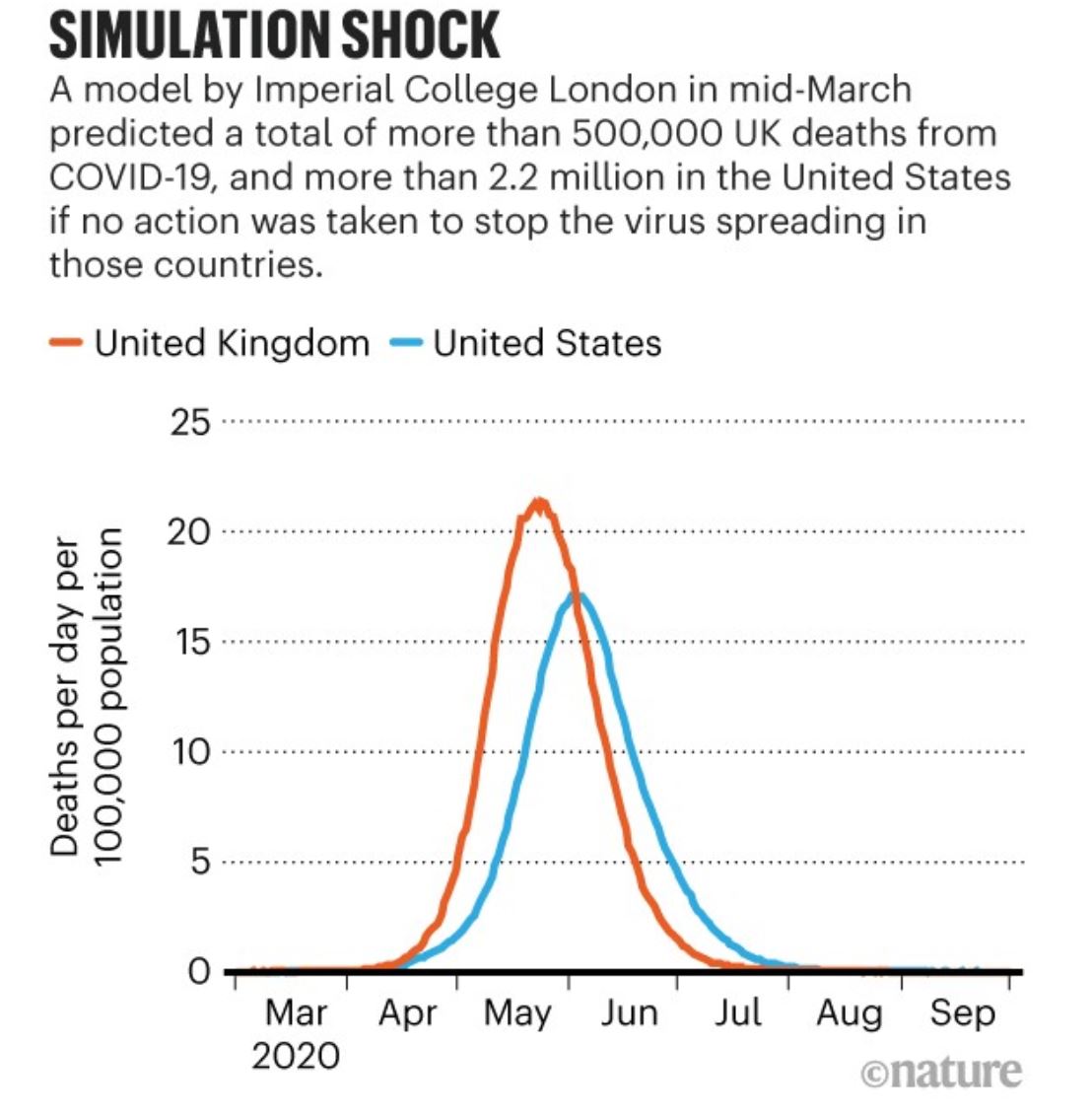
In retrospect, 2-years later, we now know it was wrong by almost an order of magnitude and just a poorly written piece of buggy code that could not be relied upon to produce the same result using the same initial conditions and random seed4. He has even admitted it himself that he got it all wrong:
And yet that model provided the basis for the draconian lockdowns and travel restrictions that the entire world endured early on in the pandemic in spring of 2020 to 'flatten the curve'. And despite that it has been discredited, lockdowns and travel bans continue to be used as strategies to limit the spread of COVID and are, with Omicron, being reintroduced once-again to 'stop the spread' and 'flatten the curve'. The Netherlands has once-again shut all non-essential businesses and closed schools until the middle of January: 'a failure to act now would likely lead to an unimageinable situation in hospitals'. Bam, everything is shut down once again for what is 'likely' (but as yet not proven and certainly disputed) and the 'unimaginable' and, thus, unproveable. There is no debate on the merits of these arguments in the public discourse, no adaptation to new facts: the narrative just evolves in precisely the direction it has wanted to go from the beginning, shuffling new facts behind the scientific sounding 'should', 'could', 'likely', 'may', 'might' language of probability, against which it is impossible to argue (these are true statements), while displacing curiosity into the domain of fantasy (and, particularly, of its horrors). And so, once again, the world rotates back into where it was almost 2-years ago to repeat everything it has already done wrong and that has, unless anyone can dispute it, NOT STOPPED THE SPREAD OF COVID.
Looking at Furguson's bell-curve now it looks like a children's doodle. Billions of people were affected by that doodle. And now, looking at the scary-looking images of Omicron, with all its 'spike' protein 'mutations', breeding in the bodies of the vulnerable, those with no capacity for self-determination, or the deviant and those with no social conscience (who knows which is implied, maybe both). The game is the same: emotionally loaded images pandering to deeply felt archetypes that provoke the fear that then makes the probabilistic language of science actually meaningful. Because of course everything is a coulda-shoulda-woulda; its the fact that something so 'unimaginable' and terrible 'could' happen that turns a 0.08% mortality rate for children under 18 among COVID deaths in the U.S.5 into a feverish hysteria to vaccinate every child, toddler, and newborn baby. It's up to a sane person to analyze the actual threat and respond to it with their wits, which is what Glenn Greenwald has argued. On the other hand, because the narrative also relies on the language of probability to hide changes in the factual context and to undermine debate, it also creates the need for an effective response to the dishonesty that is perpetuating the narrated hysteria.
The problem is that in the hidden nowhere-scape of those to whom the narrative has already been exposed as a fraud, actual debate is occurring6. And it isn't just peanuts parsing hairs. Returning to the origin story about Omicron: where it arose is actually incredibly important to ascertain. If it did arise in an immuno-compromised individual in a largely unvaccinated country, OF COURSE that should have consequences of some kind. But the fact that, as the shell game always goes, one hand behind the back, the game moves on and the origin story is largely a thing of the past means something to the street-wise. There's something there: one doesn't know what it is, but it's something.
As soon as it was clear the virus was already in Europe long before it was isolated in South Africa, could be due to its “strong genetic sequencing networks”, whatever that means exactly—but it may also be that the 'logical' fact of relying on a vaccine that does not prevent transmission of the virus could be creating large populations of rich-country citizens who, together create the conditions for the emergence of new, vaccine resistant, more virulent strains. Because that is what we have with Omicron. It may not be, as we yet don't know, more virulent in its spike-protein effects in the bloodstream (causing the thrombosis that leads to suffocation and heart-failure), but it is certainly more virulent in its spread. Where is the debate about whether or not it is the universality of the vaccination program itself that is producing these new strains? And what kinds of dangers are we creating by not only persisting according to the same COVID response logic, but intensifying it, searching out every man, woman, and child in every rich and poor country to stick a needle in?
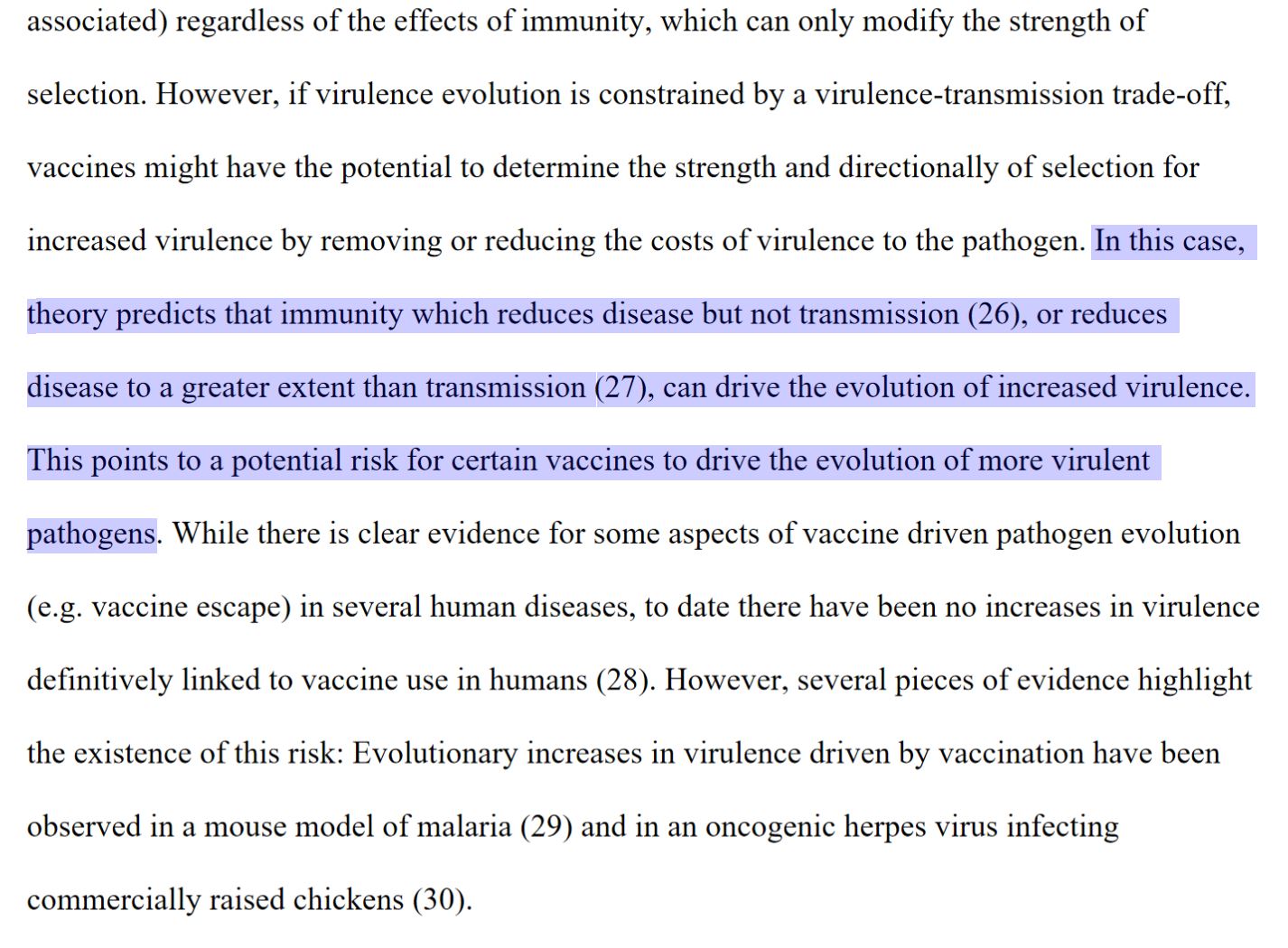
Consider this from Princeton University pre-print, non-peer-reviewed research:
Or this, from The New England Journal of Medicine:
This is what it means to learn the shell game: read the narrative to find new sources of meaning that lead to facts that are not yet available because either they cannot be available because we lack understanding or because they are being intentionally suppressed. Waiting for those who produce our discourse to have an attack of conscience, or for the guerrilla information war to finally surface new facts and to then reshape the narrative will, in the ever-increasing speed at which things are taking place, simply not be commensurate to the challenge.
Much like the provisional and improvised lives the vaccine now targets in the Global South, those of us in rich Western countries subjected to these narrative manipulations have to learn the art of the hustle. For too long life in the developed West cold be read off a script: go to college, get a job, raise a family, and die. All that has already come undone long ago, with the financial crash of 2008, and now with COVID. And partly, its disaster capitalism that arises from out of these situations: transfers of wealth upwards in bailouts to banks and corporations; but on the other hand, it is the kind of narrated existence that allows this to occur and through which we are all led, unwittingly into the processes of economic exploitation designed specifically for us, with the risks for livelihood and health they entail that are themselves of longer-term importance. These are narrative whose speed of change undermine deliberate, informed responses. In this sense, rich country citizens need to recognize that they are no longer what they once were, the terms are changed now, and an entirely new praxis for action, mode of behavior is necessary to escape the narration of their fate. Perhaps its a return to the principled Wild West character who could survive amidst the unknowns of the Frontier, adapting, thinking on his feet according to long-held principles—of one who, by liberating themselves from the stifling inhibition of fear, steps out into the world on new terms, able again to spot a friend or identify a foe, to act responsibly, cool, calm and collected under pressure. Perhaps its the return of collective thought, of the refusal to participate, to break the feedback loop that creates the possibility of rebuilding our structures of mediated thought through what means we still have. Who knows. But, whatever it is is on the knife-edge of mass-delusion, crack-pot conspiracy, and all the other viral emotionally-based hysterias that are themselves already the problem. It's not a great hand to start with, that's for sure.
Footnotes
“Community transmission and viral load kinetics of the SARS-CoV-2 delta (B.1.617.2) variant in vaccinated and unvaccinated individuals in the UK: a prospective, longitudinal, cohort study”, Singanayagam, Anika, et al; October 29, 2021; https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(21)00648-4/fulltext ↩
“Waning Immunity after the BNT162b2 Vaccine in Israel”, Goldberg, Yair, et al.; October 27, 2021; https://www.nejm.org/doi/full/10.1056/NEJMoa2114228 ↩
A new variant no surprise when rich countries hoarding vaccines, read a Guardian article headline, written by former Prime Minister of the UK, Gordon Brown. ↩
Failures of an Influential COVID-19 Model Used to Justify Lockdowns, from the Heritage Foundation; Code Review of Ferguson’s Model ↩
According to the CDC, approximately 75% all COVID deaths occur in those 65-years and higher, ~96% over 45, and only 4% under 45, the largest percentage (~26%) over 85-years. Of the almost 773,812-deaths 'involving COVID', only 621(0.08%) were in children under 18. ↩
Assessing the risk of vaccine-driven virulence evolution in SARS-CoV-2, a pre-print not yet peer-reviewed, by researchers at Princeton University (June 11, 2021); SARS-CoV-2 Variants and Vaccines, Special Report from The New England Journal of Medicine (July 8, 2021). ↩